
Group | Tuberculosis Immunology
The TB Immunology research group conducts basic research aiming to enhance our understanding of the complex host-pathogen interaction in TB with a strong focus on human immunity to TB. We also carry out translational and clinical research projects that contribute to the development of improved TB diagnosis, vaccine and host-directed therapies. Our research activities are interlaced across three complementary pillars:
- TB protective immunity
- Immunoregulation of Mtb physiology
- Immunodiagnosis of TB

Main Areas of Research
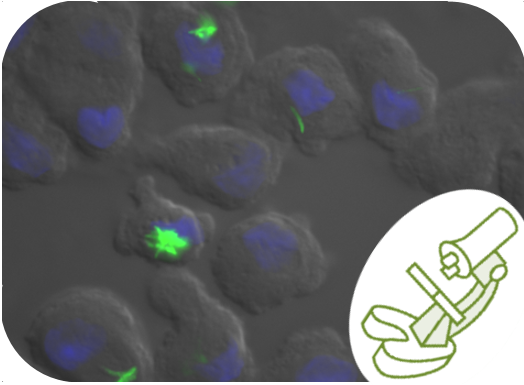
TB Protective Immunity
Human immune responses are in many instances efficient enough to prevent infection by Mycobacterium tuberculosis (Mtb). Mtb virulence relies notably on its capacity to escape the bactericidal functions of macrophages despite potentiation by NK and T cell-derived cytokines. To support the development of host-directed therapies and new vaccines against TB, we aim to understand the interplays between host-pathogen genetic traits, co-infections and environmental factors that hamper immune functions and pave the way for active TB disease.
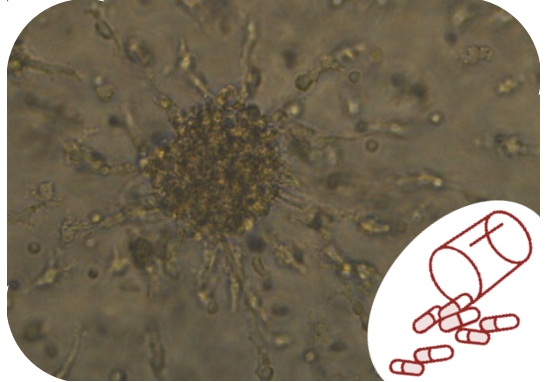
Immunoregulation of Mtb Physiology
In vitro, ex vivo and in clinico evidence are pointing towards substantial phenotypic heterogeneity across Mtb populations that can be linked to virulence traits such persistence, tolerance, reactivation and transmission. Using clinical Mtb isolates and cellular models of infection, encompassing macrophage and in vitro granuloma, we aim to dissect the contribution of individual immune cell types and their products that would favor or prevent Mtb physiological variation at the population level and influence aforementioned Mtb virulence traits.
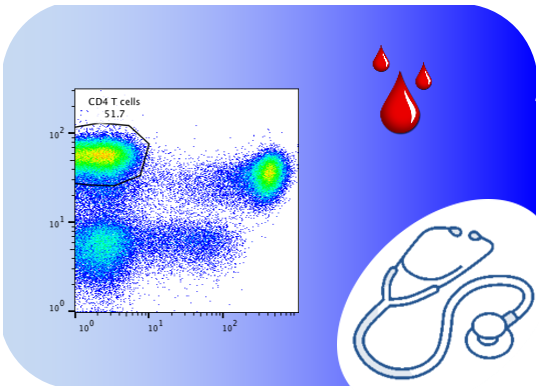
Immunodiagnosis of TB
Non-sputum based biomarkers diagnostic tools are required to overcome the paucibacillary nature and extra-pulmonary propensity of TB/HIV co-infection and childhood TB. We previously demonstrated unprecedented accuracy of an immunodiagnosis approach measuring phenotypic markers of Mtb-specific T cells by flow cytometry. We are aiming to refine and develop this assay towards a point-of-care test.
 Jasmin Albiez
Jasmin Albiez
 Damien Portevin
Damien Portevin
 Sarah Schmidiger
Sarah Schmidiger
 Laura Zaragoza Infante
Laura Zaragoza Infante